5 Policies to Create a Fair Health Care Market
March 30th, 2022
This week, actuaries with the Centers for Medicare and Medicaid projected health care spending will grow to reach almost $6.8 trillion by the year 2030 and consume nearly 20% of the country’s gross domestic product, or one in every five dollars spent. A significant portion of that spending is paid by private and public employers, which in turn, acts as a drag on both business growth and household incomes.
As innovative employers seek market solutions to wrangle health care costs while improving the quality of care they offer working Americans, they also recognize that the government has a role to play in ensuring they have a functional marketplace in which to purchase health care on behalf of their companies and employees. They have been eager to see action on the part of the Centers for Medicare and Medicaid Services (CMS) Innovation Center and Health and Human Services to help tamp down the ever-climbing health care costs that come out of their budgets – action they have yet to see.
Here are five policy areas employers want to see implemented.
1. Addressing Market Consolidation and Anti-Competitive Practices
Health care system consolidation is not a new problem, but it has gained attention over the past several years, particularly in light of a slew of megamergers proposed during the COVID-19 pandemic. In an executive order signed in July 2021, President Biden directs the Department of Health and Human Services to move forward with price transparency requirements, and directs the Department of Justice and Federal Trade Commission (FTC) to review and revise guidelines for challenging future consolidation by health systems. New guidelines would make it more likely that the FTC will intervene to stop anti-competitive mergers among health systems, improving the competitive landscape and combating rising health care costs that land on employers and other large purchasers, as well as consumers.
In addition, Congress should prohibit anti-competitive practices that have enabled some health systems to gain market power and raise prices. These practices have included anti-tiering and other contract terms that were the target of a successful lawsuit against Sutter Health System in California. The Healthy Competition for Better Care Act (S 3139), a bipartisan bill introduced by Senators Braun and Baldwin, would take on these practices. Federal legislation is also needed to prohibit drug manufacturers’ practices such as “patent evergreening” and other “patent thickets” to ensure that branded products will face healthy price competition from generic drugs and biosimilars in line with the intent of current laws.
2. Universal “Site Neutral” Payment
Medicare, along with other payers, often pay substantially more for the same care if it is delivered in a hospital outpatient department, rather than in a physician’s office, even when the service is identical. The higher payment rates put independent physician practices at a disadvantage and encourage more industry consolidation. What’s more, the higher prices charged by practices owned by a hospital system tend to be hidden from patients, causing unexpected – and often excessively elevated — out-of-pocket costs.
Universal site-neutral payments – the same pay for the same service — would save the health care system more than $350 billion (and as much as twice that) if adopted by all payers. It would also balance the playing field for independent physician practices.
3. Support for Physician-Led Accountable Care Organizations and Alternative Payment Models
All the evidence suggests that physician-led Accountable Care Organizations and alternative payment models, including those that pay clinicians prospectively to manage patient care, are more successful than hospital or payer-led models. Large employers and purchasers are interested in seeing CMS take an active hand in promoting these efforts. Policymakers can support the success of physician-led ACOs by helping them create the infrastructure needed to take on financial risk, invest in high-value care and develop partnerships with other organizations to provide comprehensive care. This includes providing financial incentives for quality performance to encourage providers to redesign care to improve health outcomes. CMS and leading payers need to communicate clear outcomes objectives and attach significant rewards and penalties providers’ performance.
In addition, a recent PBGH survey of large employers found that nearly six in 10 see low investment in primary care as a barrier to better employee health. Roughly 90% said they would be in favor of reallocating funds to primary and preventative care. One way to finance this effort, which employers would like to see CMS support, is to redirect money paid to health plans for care coordination to physician practices engaged in advanced primary care.
4. Renewed Push for Build Back Better – Including Prescription Drug Price Relief
President Biden’s nearly $2 trillion Build Back Better (BBB) proposal included provisions on drug pricing, but the effort was stymied. On Jan. 19, 2022, President Biden suggested in a press conference that the Senate would break the BBB bill into pieces, attempting to pass provisions that have support of all 50 Democratic Senators.
The current legislation would allow Medicare to negotiate on the price of certain high-cost sole-source drugs after their patent and market exclusivity periods have expired. It would also impose strict inflation caps on all high-cost sole-source drugs. Importantly, those inflation caps would apply to all purchasers, not just Medicare. If enacted, this provision would save employers, other health care purchasers and consumers tens of billions of dollars over the next decade.
5. Holding Drug Makers and Third-Party Organizations Accountable for Drug Prices
Policymakers have been looking at opportunities to increase transparency and accountability of pharmacy benefit managers (PBMs) and others in the drug supply chain. The Trump Administration’s Transparency in Coverage rule, which is being implemented by the Biden administration, albeit on a somewhat delayed timeframe, includes significant new drug price transparency requirements of health plans and PBMs. Not surprisingly, the Pharmacy Care Management Association (which represents PBMs) has sued the administration to stop implementation of certain sections of the rule. If implemented, the rule would require PBMs to report on negotiated rates and historical net prices for covered prescription drugs. Combined with the Consolidated Appropriations Act (CAA), which ultimately requires PBMs to provide the information employers need on prescription drug spending to meet their obligations under the law, would be impactful.
Importantly, no explicit statutory authority exists for policymakers to regulate PBMs directly. What is needed is for policymakers to establish direct oversight authority for PBMs in all markets. AND we need PBMs to be held to the same fiduciary standards that self-funded employers are held to. Only then will we get the accountability we need.
5 Federal Policies for Employers to Watch in 2022
January 28th, 2022
Federal policymakers, like the general public, are desperately searching for an end to the COVID-19 pandemic and a return to normality. However, with the country in its fifth wave of coronavirus cases and hospitals full to the point of breaking, the ongoing pandemic clouds and shapes the health policy landscape. Here are the five federal policy areas employers and purchasers should watch in 2022:
1. COVID Regulations and Legislation Affecting Employers
In 2020, Congress required health plans to cover the cost of COVID diagnostic testing when administered by a clinician, but the law did not set a maximum price for COVID testing, leading to sporadic price gouging. More recently, the Biden Administration finalized guidance requiring health plans to cover up to eight at-home tests per person per month. The guidance allows health plans to set a maximum reimbursement of $12 per test for tests bought over-the-counter if the plans also provide free tests to enrollees. Employers, health plans and vendors have acted quickly to implement the rule, but some employers have expressed concerns about implementation, price gouging and the overall cost to employers, which would exceed $4,000 for a family of four over 12 months. We are urging the administration will continue to revise the guidelines based on feedback from employers.
It has now been more than ten months since enactment of the American Rescue Plan Act – the last major COVID relief legislation. Congressional leaders have floated the possibility of another COVID relief bill. Specific provisions have not yet been identified, but it seems likely that it would provide economic relief to struggling businesses, including health care providers. PBGH has recommended that any further health care provider relief be tied to a moratorium or limits on mergers and acquisitions, which have historically increased costs without a corresponding increase in quality. Large employers and their employees have been forced to pick up the tab for an increasingly consolidated market.
2. A Renewed Push for Build Back Better – Including Prescription Drug Price Relief
President Biden’s nearly $2 trillion Build Back Better (BBB) proposal included provisions on drug pricing, but the effort was stymied by concerns from Sen. Joe Manchin (D-WV), who announced in late December 2021 that he would not vote for the bill as currently constructed. Senate Democratic leaders have left open the possibility of coming back to BBB later this year.
On Jan. 19, 2022, President Biden suggested in a press conference that the Senate would break the BBB bill into pieces, attempting to pass provisions that have support of all 50 Democratic Senators. The timing of this effort is unknown, but likely in the next several months.
Happily, for employers and purchasers, Sen. Manchin’s opposition to the bill is unrelated to the provisions on drug pricing. Not only has Sen. Manchin expressed continued support for meaningful drug pricing reform, but he has also suggested he would prefer the provisions be strengthened to encompass more high-cost drugs. The current legislation would allow Medicare to negotiate on the price of certain high-cost sole-source drugs after their patent and market exclusivity periods have expired. It would also impose strict inflation caps on all high-cost sole-source drugs. Importantly, those inflation caps would apply to all purchasers, not just Medicare. If enacted, this provision would save employers, other health care purchasers and consumers tens of billions of dollars over the next decade.
3. New focus on PBMs and Drug Supply Chain
Policymakers have been looking at opportunities to increase transparency and accountability of pharmacy benefit managers (PBMs) and others in the drug supply chain. The Trump Administration’s Transparency in Coverage rule, which is being implemented by the Biden administration, albeit on a somewhat delayed timeframe, includes significant new drug price transparency requirements of health plans and PBMs. Not surprisingly, the Pharmacy Care Management Association (which represents PBMs) has sued the administration to stop implementation of certain sections of the rule. If implemented, the rule would require PBMs to report on negotiated rates and historical net prices for covered prescription drugs.
Separately, the Consolidated Appropriations Act (CAA), enacted in December 2020, requires self-insured employers to report on drug costs. Specifically, the CAA requires them to report the 50 most frequently dispensed prescription drugs, the 50 most costly prescription drugs to the employer’s plan and the 50 drugs leading to the greatest increase in cost for the plan during the previous year. Further, they must submit information regarding the impact on premiums of rebates, fees and other renumeration to drug manufacturers. While the CAA’s new requirements don’t directly call out PBMs, ultimately PBMs will be required to provide the information employers need to meet their obligations under the law.
Lawmakers are now discussing whether to directly require PBMs to report on drug price information to federal authorities. Even more aggressively, some lawmakers are considering legislation that would extend fiduciary responsibilities to PBMs and other contractors of group health plans. This would go a long way to holding drug supply chain “middlemen” accountable for ensuring drug discounts are passed on to employers, other health care purchasers and consumers.
4. Addressing Market Consolidation and Anti-Competitive Practices
Health care system consolidation is not a new problem, but it has gained attention over the past several years, particularly in light of a slew of megamergers proposed during the COVID-19 pandemic. In an executive order signed in July 2021, President Biden directs the Department of Health and Human Services to move forward with the price transparency requirements noted above, and directs the Department of Justice and Federal Trade Commission (FTC) to review and revise guidelines for challenging future consolidation by health systems. New guidelines will make it more likely that the FTC will intervene to stop anti-competitive mergers among health systems, improving the competitive landscape and combating rising health care costs that land on employers and other large purchasers, as well as consumers.
Congress has also taken notice of the problem. Last fall, Sens. Mike Braun (R-IN) and Tammy Baldwin (D-WI) introduced legislation to ban anti-competitive contracting practices between hospitals and health plans. Their bill, the Healthy Competition for Better Care Act, would bar health plans from entering into contracts that include anti-competitive provisions, including “anti-tiering / anti-steering” and “all-or-nothing” requirements.
5. Post-COVID Telehealth Policy
Many policymakers and other stakeholders are actively considering overdue changes to telehealth policy. Responding to the closure of in-person settings early in the pandemic, Congress and the Administration reacted swiftly by waiving many telehealth restrictions, which are now beginning to expire.
Many bills have been introduced in Congress on telehealth over the last year, and there appears to be a growing consensus around addressing several key issues. Importantly for employers, lawmakers are considering options to allow telehealth services to be delivered across state lines. Currently, state licensing requirements limit the ability of clinicians to deliver telehealth to people outside of the state in which they are licensed. Revising licensing requirements could significantly increase the number of telehealth providers available to employees and their ability to shop around for the services they need.
Congress Must Keep Its Promise to Lower Drug Costs for All Americans
October 26th, 2021
The Danger:
The reconciliation bill currently being debated in Congress would reduce future prescription drug costs for everyone in the United States. It does this by limiting how much drug makers can raise prices for medications that have no market competition. Some members of Congress seem to think only people on Medicare deserve lower drug costs and are working to eliminate price protections for working Americans younger than 65.
The reconciliation bill in its current form would save employers and Americans with private health insurance nearly $250 billion over 10 years.* But if Congress only applies cost savings to people on Medicare, 180 million Americans will get no relief from high drug prices, and may be left to pay even more.
The Drug Companies Told Us They’ll Raise Prices:
Economists continue to debate the extent to which drug makers would increase prices for working Americans to make up for the profits they’ll lose if drug prices are reduced only for Medicare and not private insurance — a practice called “cost-shifting.” But PhRMA already told us in formal comments to the Department of Health and Human Services drug manufacturers would likely increase prices in the commercial market:
“… Government experts found that proposals to extend Medicaid rebates to other government programs will likely increase Medicaid spending and negatively affect other drug payers, such as employers in the commercial market.”
A Call for Congress:
Congressional leaders have made public promises to bring down prescription drug costs for all Americans. They need to keep those promises. Any drug price legislation must protect working people and their families, not just those with Medicare coverage. Americans with private insurance are already paying too much for their prescription drugs and need relief.
* EmployersRx estimate based on analysis by Council for Informed Drug Spending Analysis, with inflation caps based on drug prices in 2021.
cidsa.org/publications/federal-revenue-generated-by-extending-drug-price-inflation-caps-to-the-commercial-market
About EmployersRx:
The Employers’ Prescription for Affordable Drugs (EmployersRx) is a coalition of the Purchaser Business Group on Health, National Alliance of Healthcare Purchaser Coalitions, The Erisa Industry Committee (ERIC), American Benefits Council, Silicon Valley Employers Forum and HR Policy Association. EmployersRx supports public policies that drive down the cost of drugs while preserving true innovation as part of a value-based health care system. Learn more at EmployersRx.org.
The Real Cost of Health Care: Hospitals Dragging Their Feet on Price Transparency
May 17th, 2021
This year’s landmark federal rule requiring the nation’s 6,000 hospitals to begin making pricing data available publicly was supposed to help consumers and purchasers shop more intelligently for health care services. But whether that’s actually occurring seems questionable.
According to news reports and PBGH’s own analysis, wide variation in how hospitals are presenting price information make provider-to-provider comparisons difficult. Worse yet, hundreds of hospitals have coded their price lists in ways that ensure the data is invisible to Internet search engines. The Wall Street Journal reported the practice is so widespread among both hospitals and payers that the Centers for Medicare and Medicaid Services (CMS) recently issued guidance prohibiting it.
Only 35% of hospitals complying
Then there are the hospitals that haven’t complied with the transparency rule at all, apparently willing to accept a $300-per-day financial penalty in lieu of publishing their price lists. A recent study in Health Affairs found that 65 out of 100 hospitals sampled were “unambiguously non-compliant.”
Among those that have posted prices, the numbers frequently have sparked more questions than answers. Case in point: Prices for caesarean sections provided by Sacramento-based Sutter Health varied by a factor of 10—from $6,241 to $60,584—depending on which Sutter facility did the procedure and/or which insurance company paid for it.
Hospitals point to COVID-19 challenges
The transparency final rule, which was initially published in December 2019, codified an executive order issued by President Trump the previous June that had identified hospital price transparency as a means of encouraging provider competition and reducing costs. The American Hospital Association (AHA) filed suit to block the rule’s implementation and sought an emergency stay, but a federal judge upheld the legality of the regulation in December 2020 and the law took effect on January 1.
The rule requires hospitals to post their entire list of standard charges, or chargemaster, along with discounted cash prices, payer-specific negotiated prices, and de-identified minimum and maximum negotiated charges. They also must publish pricing for 300 specific shoppable health services, 70 of which have been predefined by CMS.
Hospitals believe the Department of Health and Human Services (HHS) should exercise discretion in enforcing the rule, given the challenges facilities face due to COVID-19. Insurers, for their part, have argued that the rule will cost them vastly more than anticipated, require the sharing of trade secrets, and compel the disclosure of “staggering” volumes of data.
But key elected officials are not in a sympathetic mood. Bipartisan members of the House Committee on Energy & Commerce in mid-April urged the HHS to conduct vigorous oversight and enforce full compliance. They suggested the possibility of increasing the civil penalty amount and conducing regular hospital audits. Notably, the current penalty of $300 per day, or $109,500 annually, amounts to about 0.0033% of the average hospital’s net patient revenue of $334.5 million in 2018.
A vital tool for purchasers
The price transparency rule was primarily envisioned as a tool to help consumers make better purchasing decisions. But it will likely prove most valuable to health care purchasers and employers, assuming standardized, accurate pricing data eventually is available nationwide.
That’s because the lack of visibility into pricing historically has been a source of enormous frustration for employers. Without pricing or care quality information, purchasers are effectively flying blind when it comes to decisions about employee health benefits. This knowledge vacuum has been exacerbated by gag clauses and other tactics some providers have used to prevent payers from sharing price or quality information with purchasers.
Equipped with payer-specific discounts and the other details required by the rule, purchasers should be able to determine:
- How their contracted hospitals compare on price with other hospitals, both overall and on an item-specific basis
- Whether payers are charging self-insured employers more than fully insured customers
- Whether their third-party administrator (TPA) is securing the best available deal
Greater hospital transparency could also contribute to improved health plan and pharmacy benefit management pricing visibility.
A multi-pronged approach
As important as price transparency is, it represents only one tool for addressing the enormous problem of over-priced, variable-quality health care. New payment models that align Medicare and Medicaid with private sector purchasers are necessary to ensure that efficiency and quality are consistently prioritized across the system.
And while well-functioning markets continue to represent the best way to get lower prices and higher quality, policymakers need to revise marketplace rules to ensure that drug manufacturers, hospitals and physicians don’t use anti-competitive practices to gain market power and raise prices.
Finally, protecting patients from surprise medical billing must be a key priority. Certain physician groups, often backed by private equity firms, can’t be allowed to exploit their monopoly positions to extract high prices from health plans and self-insured employers.
Democrats Gamble on Two Budget Reconciliation Bills
February 17th, 2021
Faced with Republican resistance on the size and scope of their proposed COVID-19 response legislation, the $1.9 trillion American Rescue Plan, Capitol Hill Democrats are attempting to do something no Congress has succeeded in doing since 2006 – pass two budget reconciliation bills in a single year – a particularly difficult challenge given Democrats controlling both chambers by the narrowest of margins.
The budget reconciliation process is designed to expedite consideration and passage of certain types of legislation – namely, those that impact the federal budget deficit. Unlike most other legislation, budget reconciliation bills cannot be filibustered in the Senate, meaning they can pass with a simple majority. In general, this means that the party with the Senate majority can pass the legislation without relying on bipartisan support. The rules around passage of budget reconciliation legislation are complex, but most importantly, all of the bill’s provisions must directly impact federal spending, meaning many policies of interest are off the table.
Congress is already well on its way to passing the American Rescue Plan, which was considered by committees of jurisdiction last week and is expected to be passed by the House this week. The legislation includes several priorities identified in a PBGH-led letter signed by more than 25 employer / purchaser organizations, including increased funding for production and distribution of COVID tests, vaccines and personal protective equipment. In addition, the bill provides subsidies for laid off or furloughed employees to cover 85% of COBRA premiums. The Congressional Budget Office estimates that the COBRA subsidies will help provide continuous coverage for 2.2 million people. Unfortunately, the American Rescue Plan fails to address other priorities identified by employers and purchasers, including capping prices on vaccines, testing, PPE and COVID services, and policies to increase the availability of telehealth both during and after the pandemic.
Following expected House passage next week, the American Rescue Plan will likely be taken up immediately by the Senate and could pass in a matter of weeks. Congressional leaders have set March 14 as an unofficial deadline for enactment, as that is when current funding for enhanced unemployment insurance payments is set to expire.
Congressional Democrats will likely have a heavier lift passing their second reconciliation bill later this year. While the American Rescue Plan is focused on COVID response and relief and thus enjoys strong public support, the next bill will potentially incorporate many unrelated priorities, including health care policy, infrastructure spending and tax reform. It is as part of that bill that congressional leaders have said they will seek to move more controversial health care priorities, including new coverage options, such as expansion of Medicare or a public option, and policies to bring down drug costs by allowing Medicare to negotiate for the price of brand-name drugs and to cap inflation on existing drugs.
While reconciliation’s rules mean that Democrats could avoid having to negotiate with Republicans on these priorities, it would require unanimous support among all 50 Senate Democrats to be enacted – a difficult task under all circumstances.
Last-minute talks pushed surprise billing ban across finish line
January 22nd, 2021
Unlike their 2019 failure, lawmakers this year succeeded in sealing the deal by including language in the massive COVID relief and federal spending package that President Donald Trump signed into law on Dec. 27. The surprise billing ban takes effect in 2022.
Learn More: Modern Healthcare
2021 Health Policy Priorities: Bipartisanship the Only Path to Success
January 19th, 2021
Beginning on Jan. 20, Democrats will hold a “trifecta” – control of the White House, Senate and House of Representatives – for the first time since Barack Obama’s first term in 2009.
Democrats have signaled that they intend to pass major health care legislation this year. While health care legislation has been the flashpoint of major partisan battles in recent years – most notably the passage of the Affordable Care Act in 2010 and its attempted repeal in 2017 – there is a real window for bipartisan support on legislation focused on reducing health care costs and improving quality. Over the past decade, the rate of inflation for medical services has averaged nearly 3% annually – roughly twice the rate of inflation for all other products and services. Unsurprisingly, recent public polling demonstrates that lowering the cost of care for individuals is the most popular health policy among voters. As the largest purchasers of health care, large employers know well the impact of the relentless increase in health care costs on their businesses and on their employees.
Post-COVID 2021 Policy Priorities for Large Employers
Like policymakers, employers are focused right now on stemming and ultimately defeating COVID-19. Once the pandemic is largely over, they will look to policymakers to pivot quickly to directly tackle high health care costs, inadequate quality and stubborn inequity in health care. But that does not mean it will be easy. Truly addressing the underlying problems in our health care system means directly challenging entrenched interests that perpetuate the broken status quo. That’s why taking on these issues can and should be bipartisan in nature.
Large private employers and public health care purchasers will be watching the actions of the Biden administration and new Congress with special focus on the following issues:
1. Broken Health Care Markets
Our health care system is rife with economic distortions, including inadequate competition, opaque pricing, uninformed consumers and a lack of actionable measures of quality. Large employers are interested in the changes policymakers will make to strengthen competition and transparency. Where markets have failed entirely or where there is no market, federal policymakers have a responsibility to directly manage prices, with an emphasis on strengthening competition via:
- Stronger health care anti-trust enforcement, including prohibitions on anti-competitive practices, to address the problems of industry consolidation, market power and high prices.
- Price transparency at the individual, health plan and provider levels, including unveiling negotiated prices between providers and health plans.
- Policies to increase healthy price competition among brand name drugs, generics and biosimilars
In highly consolidated health care markets, where dominant health systems have already driven up prices, it may be impossible to reinstate healthy competition. This may be particularly true in rural areas with very limited numbers of hospitals and physicians. In such cases, the federal government should directly set or constrain prices for all purchasers at fair and reasonable levels.
For pharmaceuticals with no effective competition (including many brand-name drugs under patent and/or market competition) the federal government should negotiate fair and reasonable prices available to all payers, as well as institute caps on inflation for prescription drugs currently on the market.
2. Rapid Acceleration of Payment Reforms from Fee-For-Service to Value-Based Models
Policymakers have long recognized that the fee-for-service payment system promotes higher volumes of care without accountability for the quality of care or patient experience. It is time for leaders to insist on the rapid adoption of value-based payment models for both public and private payers.
Population-based payment models, as described in the Health Care Payment Learning and Action Network’s framework, are the best way to provide flexibility to physicians and health systems while ensuring accountability for the total cost of care. The payment models must also include accountability for quality, patient experience and equity.
In the wake of the pandemic and the rapid rise of and need for remote care options, it is important to note that population-based payment models provide the right incentives for the expanded and appropriate use of telehealth services.
3. Adoption of Robust Performance Measurement with Focus on Health Equity
The ability of our health care system to deliver higher quality outcomes depends on the adoption of standardized and mandatory performance measures. Such measures are essential to the widespread adoption of value-based payments.
Performance measures should include clinical outcomes, patient-reported outcomes, appropriateness and equity. And they should be standardized and required for all physicians, hospitals and other clinicians to provide useful comparable information to patients, consumers and purchasers.
For too long, however, health care quality measures have failed to address underlying racial, ethnic and other disparities in health care. Performance measures should include the capture of racial and ethnic identification data. Further, quality improvement initiatives should focus on areas of greatest disparities, such as maternal and infant care and COVID.
Each of the policies described has enjoyed bipartisan support in the past. With just 50 Senators caucusing with Democrats and a five-seat majority in the House, the most viable path toward legislative success rests on bipartisanship.
For more on what large employers are prioritizing in 2021, read 7 Large Employer Health Care Priorities to Watch in 2021.
5 Health Care Provisions in the COVID Relief Bill Impacting Employers and Families
December 21st, 2020
Over the weekend, congressional negotiators reached a deal on a more than $900 billion COVID-19 relief package. This legislation will be tied to a year-end government funding bill. Among the many provisions in the bill are several of particular interest for employers and health care purchasers.
Below is a summary of the critical items of interest:
1. Surprise Medical Bills
After a two-year legislative fight, Congress is poised to finally pass legislation to ban surprise medical bills.
Consumer protections: If a covered individual receives out-of-network care without their consent (whether in an emergency or non-emergency situation), the individual will only be expected to pay their normal in-network cost sharing amount.
Negotiation between providers, insurers: The remaining balance of the bill will be negotiated between the health insurer and the provider. The two parties will have 30 days to negotiate a mutually agreeable payment rate. If they fail to reach agreement after 30 days, either party may request an independent dispute resolution process (IDR). Under IDR:
- Both parties will submit a “best final offer” to an independent arbitrator.
- Both parties may submit additional information justifying their offer, but the arbitrator is banned from considering providers’ billed charges and the payment rate from public payers, including Medicare. Further, the arbitrator must consider the median in-network payment rate for the service in the geographic area.
- Using “baseball style” arbitration, the arbitrator must choose one of the two offers.
- The arbitrator’s decision is final. The losing party is responsible for payment of the IDR cost.
Most care settings affected: The surprise medical bill protections apply to inpatient hospitals settings and outpatient care in emergency departments, outpatient clinics and surgical centers and clinician offices. They also apply to air ambulance transport. Unfortunately, they do not apply to ground ambulance transport services.
2022 implementation: Protections against surprise bills will take effect for health plan years beginning on or after January 1, 2022.
Impact: The consumer protections included in the legislation will put an end to the scourge of surprise medical bills and reduce the ability of certain providers from driving up costs by implicitly threatening to bill patients if they are not included in insurance networks. However, there is concern that the IDR process may be “gamed” by providers and will be less successful at holding down costs for purchasers than the proposed alternative of a benchmark payment rate for surprise bills. Nevertheless, the Congressional Budget Office and other independent analysts believe that the legislation’s requirement that the arbitrator consider the median in-network payment amount will be effective at holding down costs.
2. Health Care Price Transparency
No more gag clauses: The final bill will ban “gag clauses” from health plan/provider contracts. These clauses prohibit plans from disclosing to plan sponsors and individuals’ financial information including the allowed amount and provider-specific negotiated payment amounts for items and services covered by the health plan.
Drug spending disclosures: The bill also requires annual disclosure by health plans regarding spending on prescription drugs, including the most frequently dispensed drugs, the highest cost drugs, the drugs with the fastest rising spending and the effect of drug rebates, fees and other renumeration plan premiums.
Impact: The ban on gag clauses in provider/plan contracts will provide meaningful, provider-specific information to plan sponsors and individuals regarding prices. However, Congress chose not to include accompanying legislation that would give plan sponsors the tools they need to use this information to stop dominant health care systems from engaging in anti-competitive behavior. This will, unfortunately, allow health systems to continue to drive up costs for purchasers and consumers without improving quality.
In addition, Congress chose not to include meaningful reform to the way in which health plans and pharmacy benefit managers (PBMs) purchase drugs. Previously considered legislation would have provided drug-specific price disclosures, discounts and rebates, and banned PBMs from engaging in “spread pricing,” in which the PBMs directly profit from rebates and discounts they negotiate rather than passing them onto plan sponsors. Instead, the final language in the bill provides only high-level aggregated information without a ban on spread pricing. It is unlikely the legislation will result in any change in behavior by PBMs and health plans.
3. Direct Economic Relief
Stimulus payments: Up to $600 per person in direct stimulus payments to individuals, phasing out for families with income exceeding $75,000.
Increased financial support: Enhanced unemployment insurance benefits of $300 per week for up to 11 weeks.
Help for small business: $240 billion for Paycheck Protection Program loans for small businesses, including non-profit organizations. Qualifying PPP recipients will need to demonstrate significant revenue losses in 2020.
Impact: The enhanced unemployment insurance and extension of the paycheck protection program will help struggling families and keep the economy afloat during the pandemic. However, Congress did NOT include COBRA subsidies for employees who have been laid off or furloughed – many of whom have joined the ranks of the uninsured since the pandemic began. These subsidies would have provided important financial support and medical continuity for families affected by job loss.
4. COVID Response
The bill provides additional fund for vaccines and COVID testing practices intended to help get the pandemic’s spread under control.
Vaccines: $20 billion for purchase of vaccine doses by the federal government; $8 billion for vaccine distribution
Testing: $20 billion for states to conduct testing and contact tracing
Provider relief: $20 billion in additional economic relief for health care providers.
Impact: The COVID response funding made available under this bill is critical to helping the country exit the pandemic as swiftly and effectively as possible – the necessary step to reinvigorating the economy.
5. Flexible Spending Account Rollover
The legislation allows flexibility for taxpayers to rollover unused amounts in their health and dependent care flexible spending arrangements (FSAs) from 2020 to 2021 and from 2021 to 2022. It also permits employers to allow employees to make a 2021 mid-year change in contribution amounts.
Impact: This provision gives employers and employees flexibility in managing unexpected changes in health care costs during the pandemic.
6 Things Large Employers are Watching for in the Next Round of COVID Legislation
July 27th, 2020
More than three months after enactment of the landmark CARES Act, and more than two months after the House of Representatives passed the HEROES Act – their own “Phase 4” legislation – the Senate is finally taking steps to pass another major bill responding to the still raging COVID-19 pandemic. As the likely last chance to pass major legislation before the November elections, this bill is particularly vital for employers and health care purchasers seeking to stay financially stable and manage COVID-19 costs during the sharpest economic contraction since the Great Depression.
Congressional and White House negotiations over this high-stakes (and likely more than $1 trillion) bill will dominate the headlines coming out of the nation’s capital for the next several weeks. PBGH and its employer/purchaser allies have weighed in with Congress and the Administration, including in two letters this week, focused on testing and our other priorities, signed by more than 30 national, regional, and local purchaser organizations. Here are the six employer priorities you should watch out for in the weeks ahead and the six sticking points that could spell trouble for the bill.
What Employers and Purchasers Want to See
- Stopping Price Gouging and Ensuring Fair Prices: Since the pandemic began to affect the United States in February, stories have abounded about bad actors engaging in egregious pricing of critical equipment. While largely limited to personal protective equipment (PPE) and testing, price gouging could get worse as the pandemic wears on. Of particular concern, the CARES Act, enacted in March, stipulates that all health insurance plans must cover the cost testing in full for employees without placing any limit on what a provider may charge for a test. The House-passed HEROES Act could further exacerbate the problem by mandating coverage – with no out-of-network price limitations — for all COVID-19 treatment.Large employers are urging Congress to not mandate that they cover these costs in full without appropriate guardrails to ensure fair prices for out-of-network care and testing. Further, a blanket ban on price gouging for COVID-19 supplies and services, enforceable by the Federal Trade Commission and state attorneys general, is essential to ensuring a fair and reasonable market.
- Banning Surprise Billing: Surprise billing has been a top priority for employers and purchasers for several years, and while Congress has come close to banning this egregious practice, it has not yet reached a final agreement. Recognizing that this may be their last opportunity, congressional leaders, led by retiring Sen. Lamar Alexander (R-TN), are pushing to include a ban in the upcoming bill. Sen. Alexander’s legislation would ban surprise billing while stipulating a market-based benchmark price for out-of-network care. Such a benchmark has been found to reduce health care costs over time for consumers, purchasers, and taxpayers alike.
- Providing Subsidies for COBRA Coverage: The pandemic has led to the sharpest rise in unemployment in the nation’s history. With millions of people laid off or furloughed, the number of uninsured people has spiked. Employers want to ensure the availability of direct subsidies for COBRA coverage so that laid off and furloughed workers can continue to stay on their employer-sponsored insurance without having to pay the full – and often unaffordable – premium.
- Federal Funding for Testing: Nearly six months since COVID began to spread in the United States, the country still lacks sufficient diagnostic tests to provide timely access to COVID-19 diagnosis. With obvious concern about getting the U.S. economy back on its feet, and a recognition that the health of American citizens and the economy are interwoven, large employers are looking to Congress to infuse new federal spending to ensure timely access to tests for all who need them.
- Financial Support to Struggling Primary Care Providers: Paradoxically, the pandemic has led to a significant decrease in utilization of health care, particularly for primary care providers. Many such providers are struggling to keep their doors open during the ongoing pandemic. According to survey findings from a provider survey conducted by the Larry Green Center at Virginia Commonwealth University, 40% of primary care clinicians say they may lack the financial resources to stay open through the end of August. Employers are looking to Congress to set aside a portion of funds already appropriated to the Provider Relief Fund for struggling primary care providers.
- Policies to Mitigate Risk in the Employer Health Insurance Market: While health care spending is down since the beginning of the pandemic, many patients are deferring necessary care. Faced with a possible spike in utilization next year, purchasers are unable to accurately project spending into 2021. That’s why they’re largely supporting the establishment of a one-sided risk corridor that would provide financial support to purchasers if costs substantially exceed projections.
The August recess is officially scheduled to begin on Aug. 8, but negotiators are already signaling that they may not reach final agreement by then. Hopefully, employers will have a clear indication of what is in and what is out by the middle of the month.
Congress Gets Serious About COVID Phase 4 Legislation
May 18th, 2020
To date, Congress has passed four bills to combat the threat of COVID-19:
- March 6: Coronavirus Preparedness and Response Supplemental Appropriations Act (“Phase 1”) – $8.5 billion
- March 18: Families First Coronavirus Response Act (“Phase 2”) – $200 billion
- March 27: Coronavirus Aid, Relief, and Economic Security Act (CARES Act) (“Phase 3”) – $2.2 trillion
- April 24: Paycheck Protection Program and Health Care Enhancement Act (“Phase 3.5”) – $500 billion. This bill is colloquially known as “Phase 3.5” as it was primarily a vehicle to renew and extend funding authorized in “Phase 3.”
Notice a theme?
First, the cost of the bills has increased exponentially. In the span of just three weeks in March, the amount of money Congress believed was necessary to combat coronavirus multiplied by more than 250 times. (The White House’s original request for Phase 1 was just $2.5 billion.) Even the roughly $2.2 trillion allocated under the CARES Act – to date the costliest bill enacted in U.S. history – proved insufficient, and Congress found itself having to renew funding for several programs less than a month later.
Second, the pace of lawmaking has slowed considerably. Notwithstanding “Phase 3.5,” Congress went from passing a new bill roughly every 10 days to having not funded any new programs for nearly two months. Since Phase 3 was passed in late March, however, the number of confirmed COVID-19 cases in the United States has risen from just over 100,000 to more than 1.4 million, and the number of confirmed deaths has increased from roughly 2,000 to more than 80,000. Equally concerning, the economy has gone into free-fall, with the official unemployment rate hitting nearly 15 percent, the highest figure since the Great Depression nearly 90 years ago. Economists expect the unemployment rate to continue to climb.
While some on Capitol Hill and in the administration continue to urge a “wait and see” approach, it is becoming increasingly clear that Congress will have to pass at least one more large virus response and economic stimulus bill. Unlike previous bills, which passed relatively quickly and with overwhelming support, the debate over “Phase 4” is likely to be more in line with what we have come to expect from Washington – a bitter partisan battle.
House Democrats Make the Opening Move
On March 15, the House of Representatives, H.R. 6800, the Health and Economic Recovery Omnibus Emergency Solutions Act (HEROES) Act, largely on a party-line vote. Weighing in at around $3 trillion, it roughly equals the amount of federal funding allocated so far in the four previous bills.
Spanning more than 1,600 pages and hundreds of individual provisions, the bill is particularly noteworthy for the nearly $1 trillion for state and local governments, $200 billion in hazard pay for essential workers, and allocating another round of $1,200 stimulus checks to individuals. While Republicans have already called the HEROES Act “dead on arrival,” is represents the Democrats’ opening bid in what will be a prolonged debate. It is after House passage that “real” negotiations with the White House and congressional Republicans will begin.
Republican Priorities
Republican leaders and the Trump Administration have other priorities. Republicans are split on how costly a Phase 4 bill should be. While President Trump appears to have no concerns about crafting a large bill, fiscal conservatives on Capitol Hill and in the administration are expressing alarm about the aggregate cost of COVID-19 on the federal budget. It is safe to assume the final bill will be smaller – perhaps much smaller – than $3 trillion. One area Republicans are united on is the need for businesses that reopen after stay-at-home orders are lifted to be given indemnity against lawsuits by consumers who may be exposed to COVID-19. Separately, the President has urged Congress to provide a payroll tax holiday in the next bill, though that idea has only lukewarm support among Republicans and Democrats.
What About Employers?
After passage of the CARES Act in late March, PBGH laid out a set of policy priorities on behalf of large employers with the overlying goal of helping employers continue to provide high quality health to their employees.
As noted in the chart below, the HEROES Act checks a few boxes, but there is still substantial room for improvement as we enter the coming debate.
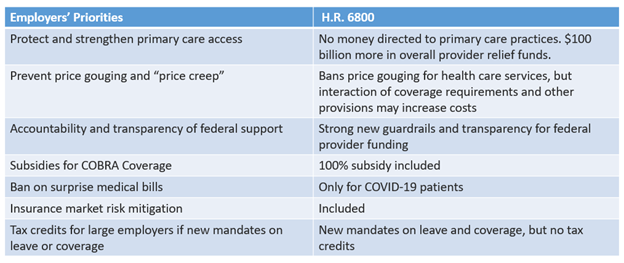
As Congressional leaders begin to work out details of the final Phase 4 bill, PBGH will be engaging with congressional leaders on each of these topics, with a particular focus on strengthening the primary care system and preventing price spikes that could fundamentally destabilize the ability of its members to continue to provide high quality coverage to their employees. And on May 19, PBGH was jointed by 35 organizations representing many of the nation’s leading private and public sector employers in issuing a letter to congressional leaders requesting they take immediate action to ensure Americans have access to high-quality, affordable health care, both now and long after the COVID-19 pandemic ends.